In the past five to ten years, the epidemiological profile of HIV in Australia has changed, underpinned by the peculiarly 21st century complexities of globalisation, mass migration and highly mobile and transient populations.
Australia has long been admired for its swift, often controversial, response to the emergence of HIV and AIDS in the early 1980s, which was characterised by cooperation between federal and state governments and advocates from groups most at risk. AIDS diagnoses peaked in 1994, and declined rapidly with the introduction of antiretroviral therapy. Very few people in Australia are now diagnosed with AIDS. HIV diagnosis rates have remained relatively low, when compared to similar countries, and, in the past few years, have stabilised at approximately 1000 people per year. Australia’s goal is for zero new HIV infections by 2020.
While the national HIV diagnosis rates are still highest in men who have sex with men, there are indications of a smaller, but significant, epidemic emerging. Over the last decade, there has been a noticeable increase in HIV diagnoses among migrant and mobile populations in Australia, which is reflective of global trends. Gay and heterosexual people, and their partners, from high HIV prevalence regions, most noticeably Sub-Saharan Africa and South-East Asia, and Australian men who travel to and from countries with high HIV prevalence, are most at risk.
According to 2015 figures from the Australian Bureau of Statistics, 28 per cent of Australians were born overseas, the highest proportion in 120 years, and the percentage of residents born overseas has increased every year for the past 15 years. Additionally, many Australians are highly mobile, travelling regularly for work or pleasure, often to countries with high HIV prevalence. In 2014-15 there were 16.9 million departures, comprising 9.2 million Australian residents departing short-term, 7.3 million visitors and 391,200 permanent and long-term departures.
Australia’s 7th national HIV strategy identifies migrant and mobile populations as priority groups in the HIV response. The issue is complicated, however, by the divergent socioeconomic and cultural drivers of the behaviours contributing to their higher HIV transmission rates. While there are currently initiatives to target these priority populations, they are typically ad-hoc or pilot in nature, and poorly coordinated or fragmented.
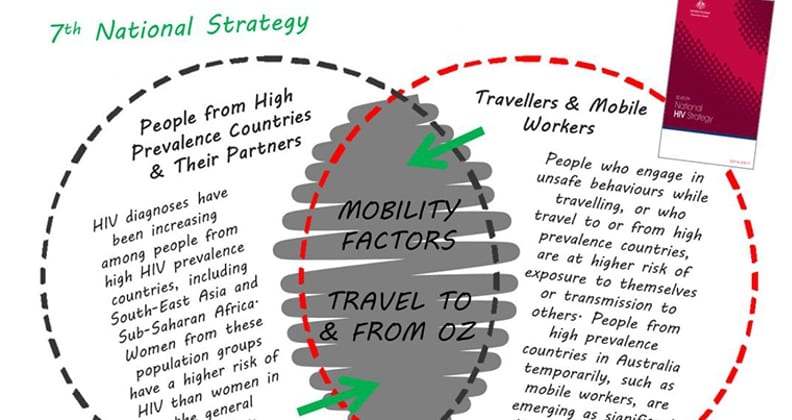
The strategy identifies migrant and mobile populations as priority groups.
In the 2014 report, HIV and Mobility in Australia: Road Map for Action, Dr Roanna Lobo, Research Fellow, Sexual Health and Blood-borne Virus Applied Research and Evaluation Network, and Ms Gemma Crawford, Research Fellow from the Collaboration for Evidence, Research and Impact in Public Health, in collaboration with colleagues from La Trobe University, examined what is required to effectively manage these new HIV epidemics.
Dr Lobo suggests context is critical to understanding the contemporary HIV landscape and developing effective strategies for emerging groups at risk of HIV transmission.
“Migrant and mobile populations are not a homogeneous group. There are very significant contextual differences between an Australian male who contracts HIV when travelling to a country with high HIV prevalence, for example, and a woman from a country in Sub-Saharan Africa, who is migrating to Australia,” Dr Lobo said.
“For the woman, barriers to testing and treatment in Australia may include visa eligibility, language, stigma and low perceived risk. By contrast, for Australian-born men who acquire HIV overseas, perceptions of risk both prior to and during travel, and the networks they participate in, both on and off line, are important.”
Ms Crawford, who is completing her PhD examining HIV risk for Australian male expatriates, and longer-term travellers, agrees.
“We need tailored, relevant strategies to reach sub groups. Disregarding variations can lead to misguided generalisations about health needs, and lower utilisation rates of health services,” Ms Crawford said.
“For travellers and mobile workers, our response must extend beyond travel campaigns and education. We may require interventions in the places that risks are happening, and we need strong links into the peer networks that may influence these risks. For migrants, increasing access to HIV testing and reducing the impact of stigma and discrimination is vital.”
While it’s clear the changes to Australia’s HIV epidemic are multi-faceted and complex, they remain poorly understood. Dr Lobo believes the paucity of surveillance data has contributed to the difficulties in developing a comprehensive understanding of, and effective approaches for, priority groups.
“Perhaps one of the most critical components for an effective public health response to Australia’s changing HIV profile is reliable surveillance data, and effective evaluation to inform funding, policy decisions and practice. Until recently, a national approach to surveillance and monitoring remained elusive,” Dr Lobo said.
Australia’s increasingly mobile and changing migrant population will play an ongoing role in the nation’s HIV epidemic. The research team at Curtin continues to lead a range of research and advocacy activities, including a national Community of Practice for Action on HIV and Mobility, to maintain momentum on the issue.